Hello I’m Dr. Lee!
Every country has a border. Some borders shift after wars or treaties. Some are redrawn by political agreements. But certain borders the ones defined by geography, by rivers, by mountain ranges have a way of reasserting themselves over time, regardless of what maps say. Your mouth has a border like that.
It’s called the mucogingival junction, and it is one of the most clinically significant boundaries in periodontics. Understanding where it sits, what it separates, and why your body works constantly to maintain it is key to understanding why gum recession treatment works the way it does — and what determines whether results last.
Two Territories, One Boundary
Think of your gums as divided into two distinct territories.
The territory closest to your teeth is tough, stable, firmly attached to the underlying bone, and built to withstand the daily mechanical forces of chewing, brushing, and speaking. This is the keratinized gingiva — the firm, pale pink tissue you can see hugging the base of your teeth. Its surface cells are hardened with a protein called keratin, the same substance that makes fingernails resistant to damage. It doesn’t stretch easily. It doesn’t tear under moderate pressure. It is the frontline defense for your tooth roots.
Below and beyond that tough zone lies the second territory — softer, more mobile tissue called alveolar mucosa. This tissue is flexible and loosely attached to the structures beneath it. It serves important functions in allowing the lips and cheeks to move freely, but it was not designed to sit right next to your teeth absorbing the forces of a toothbrush twice a day.
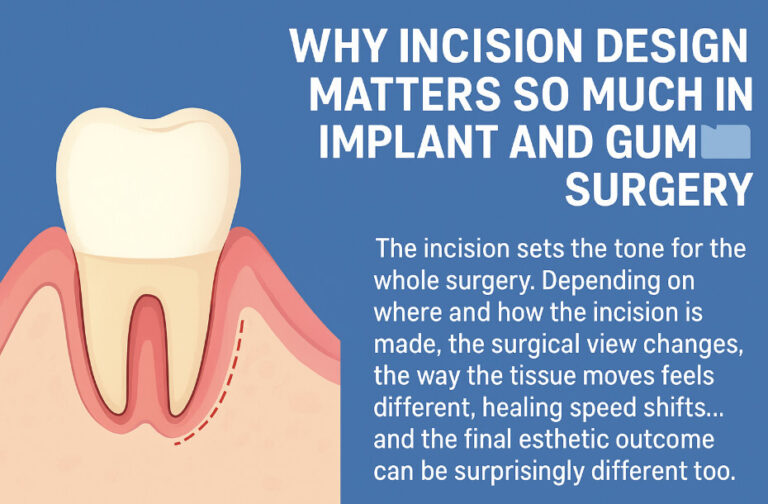
The mucogingival junction is the exact line where these two territories meet. On one side: tough and protective. On the other: soft and vulnerable.
When the Border Is in the Wrong Place
In a healthy mouth, the mucogingival junction sits well below the gum margin — leaving a comfortable band of tough tissue between the edge of the gum and the softer tissue below. That band is the buffer zone. As long as it’s wide enough, the tooth root is protected.
When gum recession occurs, the gum margin moves downward — but the mucogingival junction largely stays where it is. The result is that the buffer zone shrinks. In severe cases, the gum margin retreats all the way to the junction itself, leaving virtually no tough protective tissue at all. At that point, the tooth root sits at the edge of soft, fragile mucosal territory with almost nothing standing between it and further damage.
This is why periodontists pay such close attention to the mucogingival junction when evaluating recession. The question isn’t only how much recession has occurred — it’s how much protective territory remains between the current gum margin and the junction.
The Body’s Built-In Border Defense
Here is where the border analogy becomes most instructive. The mucogingival junction is not simply a line drawn by circumstance. Research suggests it has a genetically preferred position — a location your body actively works to maintain, and to return to when something disrupts it.
Think of it like a river forming a natural border. You can dam it, redirect it, temporarily reroute it. But rivers have a tendency to find their original course again over time. The mucogingival junction behaves similarly.
Long-term studies following patients for up to 18 years after gum surgery found a consistent pattern: regardless of where surgery repositioned the junction, it gradually drifted back toward its original pre-surgery location over the years that followed. The body does not simply accept the new position. It corrects toward the position it was always trying to maintain.
Why This Matters After Gum Surgery
This natural tendency has two very different implications depending on the direction of the surgical shift.
When gum surgery moves the junction upward — toward the teeth — as happens in root coverage procedures, the long-term drift back toward the natural position can actually be beneficial. As the junction slowly returns toward its preferred location over months and years, the band of tough protective tissue above it gradually widens. Studies have documented this process continuing for three or more years after surgery, with patients gaining meaningful additional tissue width without any further intervention.
The deeper the original recession before surgery, the greater this long-term gain tends to be. Patients with significant recession who achieve good initial root coverage often find that their protective tissue band continues improving well beyond the first year.
But the same tendency cuts the other way when the natural position of the junction is already too close to the teeth. If your mucogingival junction is genetically positioned in an unfavorable location — close to the gum margin even in the absence of recession — then after surgery, the long-term drift back toward that position may partially reverse the gains achieved in the operating chair. The border reasserts itself.
What Surgery Can and Cannot Do
This is the most important clinical takeaway from understanding the mucogingival junction. Surgery can temporarily relocate the boundary. Surgery can add tissue volume that changes how the boundary behaves. Surgery can dramatically improve the clinical situation. But surgery cannot override the body’s long-term tendency to return the junction toward its genetically preferred position.
What determines whether surgical results last is not only the technique used — it’s whether the pre-treatment position of the mucogingival junction was assessed, whether the tissue volume augmentation was sufficient to sustain the new position long-term, and whether the patient maintains the monitoring and habits that protect the result over the years that follow.
The border can be moved. Whether it stays moved is a different question entirely — and answering it honestly requires understanding the biology of the tissue you’re working with, not just the mechanics of the surgery.
What You Should Ask Your Periodontist
Before any gum recession treatment, ask your periodontist where your mucogingival junction currently sits, and what that means for the surgical plan. Ask whether the technique being proposed is designed to move the junction, add volume near it, or rely on long-term natural tissue migration to achieve the desired result. Ask what the realistic three-year and five-year picture looks like — not just the six-week post-operative result.
The mucogingival junction is a small anatomical landmark. But understanding what it is, why your body defends it, and how it interacts with the treatment you receive is one of the clearest windows into the long-term trajectory of your gum health.